What does heterogeneity mean for cancer treatment models?
Behind the papers
Cooperative adaptation to therapy (CAT) confers resistance in heterogeneous non-small cell lung cancer
Morgan Craig, Kamran Kaveh, Alec Woosley, Andrew S. Brown, David Goldman, Elliot Eton, Ravindra M. Mehta, Andrew Dhawan, Kazuya Arai, M. Mamunur Rahman, Sidi Chen, Martin A. Nowak, Aaron Goldman
Read the paperDeterminants of combination GM-CSF immunotherapy and oncolytic virotherapy success identified through in silico treatment personalization
Tyler Cassidy, Morgan Craig
Read the paper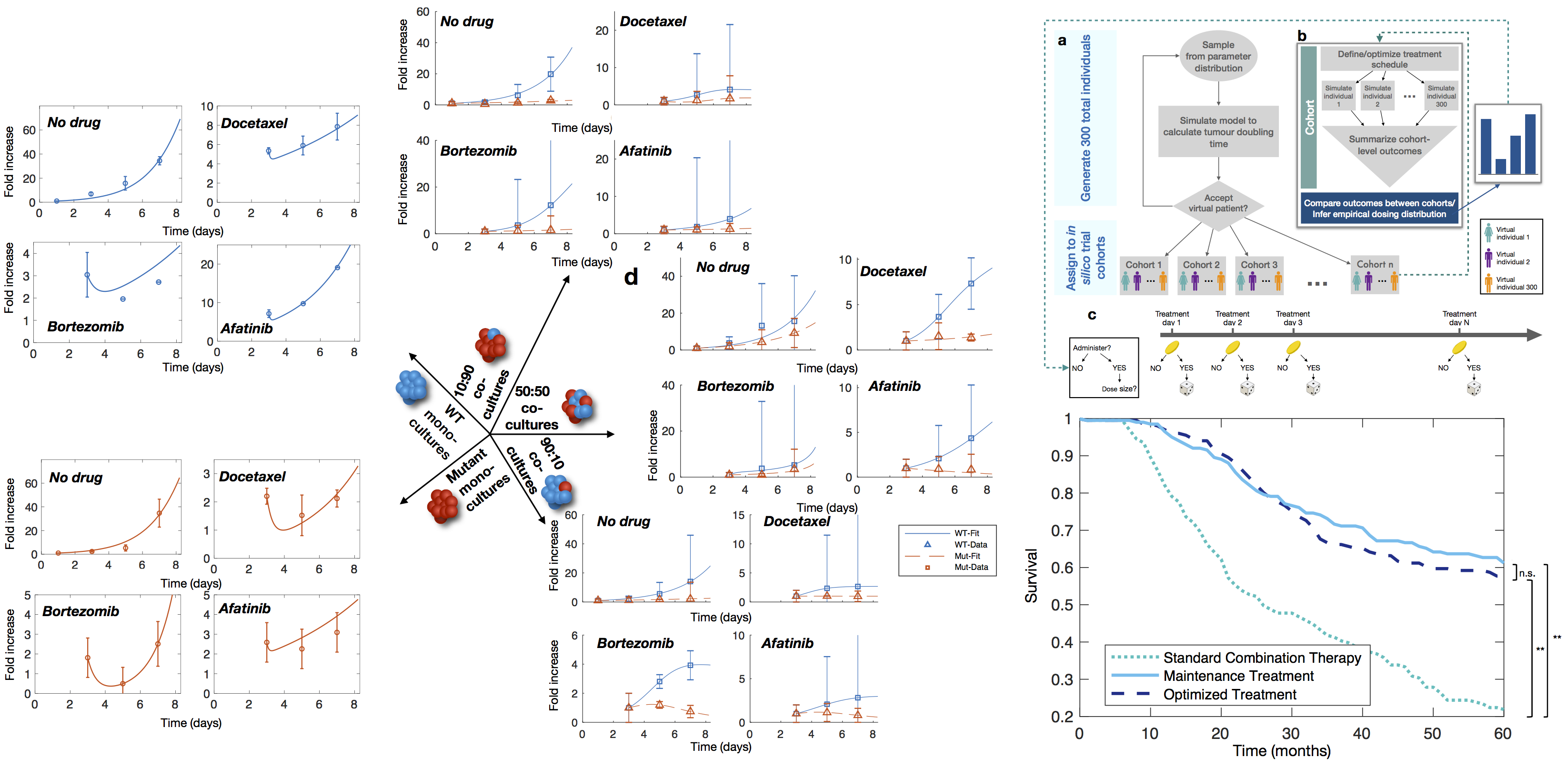
Figure 1. Incorporating heterogeneity into mathematical models of cancer treatment. Left: Growth kinetics of mono- and co-cultures in varying proportions of WT:mutants in NSCLC tumour spheroids with and without treatment. From Craig et al. 2019. Right: By expanding a cohorts of virtual patients, we optimized combination T-VEC and GM-CSF treatment and established improved therapeutic schedules for the treatment of late-stage melanoma. Adapted from Cassidy and Craig 2019.
It goes without saying that patients are heterogeneous beyond the tumour level, and interindividual variability contributes heavily to therapeutic outcomes. Drug development takes a long time and costs a lot of money. In cancer drug development, there is a success rate between 3% and 8% once a molecule enters clinical trials, which compounds these time and monetary costs. Reasons drugs may fail in the pre-clinical to clinical transition include suboptimal treatment schedules and poorly identified responders and non-responders within trial cohorts. In each of these aspects, mathematical modelling can provide a rational means to identify how best to deliver treatment and to whom we give the therapy, thus increasing the likelihood of successful trials. New immunotherapies in particular benefit from such quantitative analyses, given the high rates of failure at clinical trials despite very encouraging results in certain cancer types (including NSCLC). It is likely that immunotherapies will need to be combined with other drugs to bolster their efficacy. In this vein, we developed a mathematical model of the oncolytic virus T-VEC, which was approved by the FDA for the treatment of melanoma in 2015. Oncolytic viruses preferentially infect tumour cells, ultimately causing their destruction and eliciting an enhanced immune response against the tumour. Oncolytic virus dynamics are intrinsically linked to the cell cycle kinetics of host cells, since they hijack their mitotic machinery. Given this, our model incorporated intrinsic heterogeneity in cell cycle times for tumour cells either susceptible or resistant to immune interactions. Further, we also expanded a population of virtual patients to represent other patient-specific characteristics that were found to impact on therapeutic outcomes. Each virtual patient was confirmed to correspond to realistic disease trajectories, and twinned into independent cohorts to interrogate on optimal treatment scheduling strategies. In this way, we could identify causal mechanisms controlling outcomes, as each cohort was identical. We investigated tailored schedules of combination T-VEC and systemic immunotherapy in the form of exogenous GM-CSF, whose expression is enhanced by the oncolytic virus. We found a high degree of variability in individual schedules, however, using empirical inference, we established a cohort-level schedule that performed equally as well as the individualized one, both significantly outperforming standard combination therapies in survival while reducing the therapeutic burden to each patient (Figure 1, right). Each of these approaches highlights that models that incorporate heterogeneity, be it at the genetic level through stochastic models, with respect to phenotype-to-phenotype interactions, or patient-specific characteristics, can be deployed in clinically-relevant ways to improve how we design and deliver anti-cancer treatments. I believe the answer to the question: “What does heterogeneity mean for cancer treatment models?” is that our math onco community will continue to developed sophisticated mechanistic models, intrinsically integrated into pre-clinical and clinical pipelines, that improve our understanding of cancer biology and therapy.References
- Altrock, P., Liu, L. & Michor, F. The mathematics of cancer: integrating quantitative models. Nat Rev Cancer 15, 730–745 (2015).
- Marusyk, A., Almendro, V. & Polyak, K. Intra-tumour heterogeneity: a looking glass for cancer?. Nat Rev Cancer 12, 323–334 (2012).
- Govindan, R. et al. Genomic Landscape of Non-Small Cell Lung Cancer in Smokers and Never-Smokers. Cell, 150, 1121-1134 (2012).
- Craig M., Kaveh K., Woosley A., Brown A.S., Goldman D., et al. Cooperative adaptation to therapy (CAT) confers resistance in heterogeneous non-small cell lung cancer. PLOS Computational Biology. 15, e1007278 (2019).
- Brady, S.W., McQuerry, J.A., Qiao, Y. et al. Combating subclonal evolution of resistant cancer phenotypes. Nat Commun 8, 1231 (2017).
- Cassidy T., Craig M. Determinants of combination GM-CSF immunotherapy and oncolytic virotherapy success identified through in silico treatment personalization. PLOS Computational Biology. 15, e1007495 (2019).
- Wong, C.H., Siah, K.W., Lo, A.W. Estimation of clinical trial success rates and related parameters. Biostatistics. 20, 273–286 (2019).
- Moleirinho, M.G., Silva, R.J.S., Alves, P.M., Carrondo, M.J.T., Peixoto, R. Current challenges in biotherapeutic particles manufacturing. Expert Opinion on Biological Therapy. 20, 451-465 (2020).
© 2026 - The Mathematical Oncology Blog