Mechanistic learning in action at COMPO
COMPO (COMPutational pharmacology and clinical Oncology) is a project team, jointly affiliated to Inria – the French national institute for computer science and applied mathematics – and Inserm (French national institute for biomedical research), part of the Center for Research on Cancer of Marseille (CRCM).
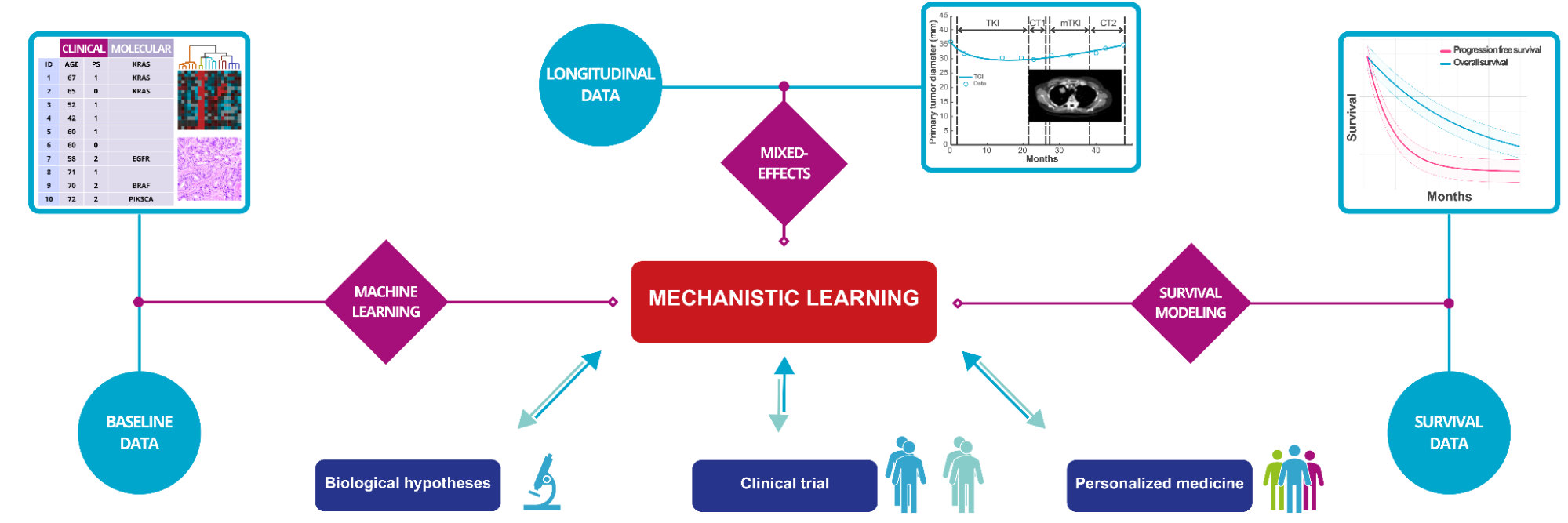
We develop novel computational models integrating data available in clinical or experimental oncology (from clinical trials, academic studies or routine care), using a combination of mechanistic modeling (i.e., models that simulate the pharmaco-patho-physiological processes dynamics) and statistical (machine) learning, that we term mechanistic learning[1]. The main goals are: 1) to develop personalized medicine, 2) to assist clinical trials (design of scheduling regimen, anticipation of final results) and 3) to use mechanistic modeling to test biological hypotheses and improve our understanding of pharmaco-patho-physiological processes in cancer. To achieve this, the team uniquely gathers 4 tenure mathematicians, 4 tenure pharmacologists and 5 medical oncologists within the same research unit.
From PK/PD modeling to a model-driven clinical trial
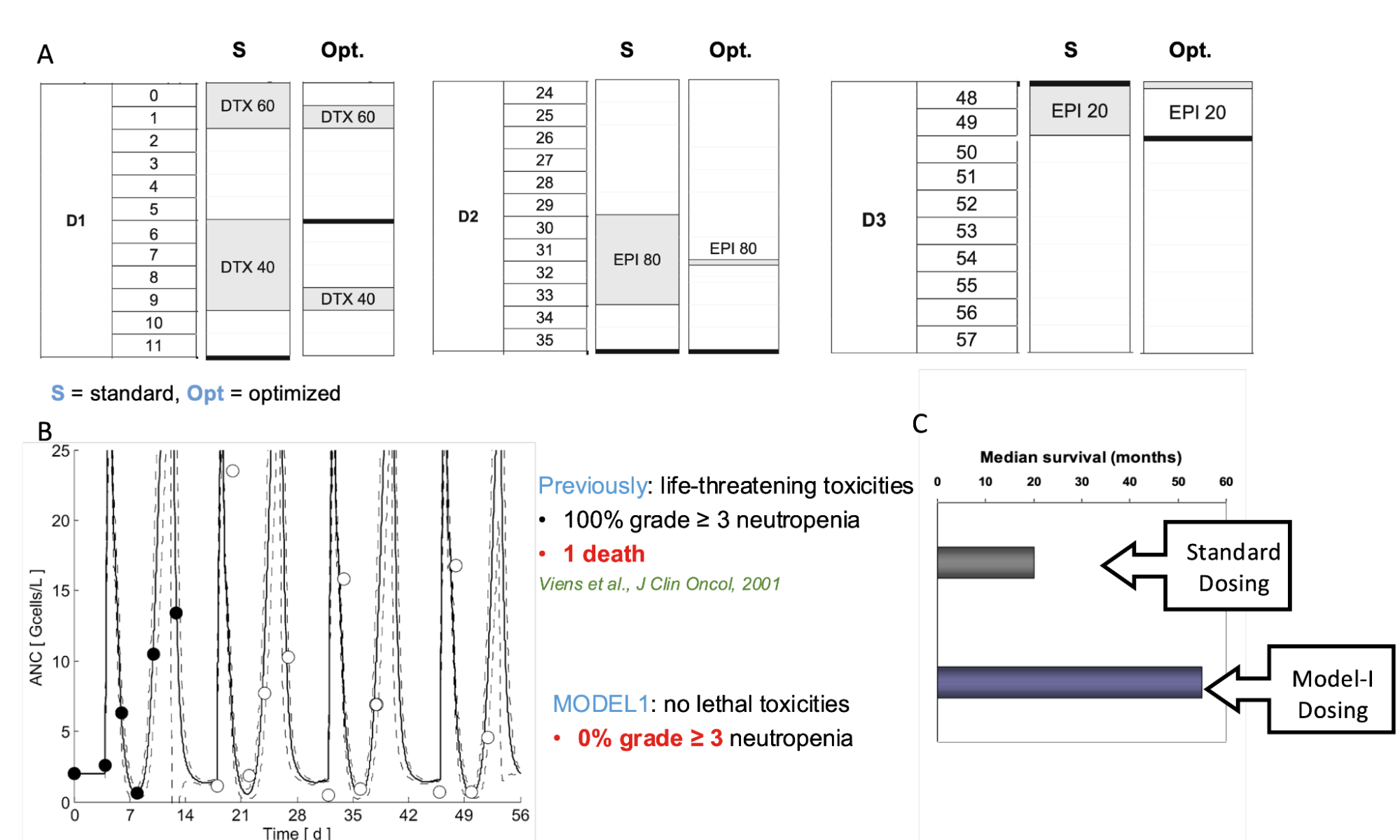
The team is historically grounded into pharmacokinetics / pharmacodynamics modeling with pioneering work from automatic engineer Pr Iliadis in the early 1990's[2]. Further joined by mathematician Pr Barbolosi, they designed the first mathematical modeling-driven clinical trial (Figure 2)[3,4,5]. This phase 1/2 study aimed at guiding the intensification of combined chemotherapy regimen in metastatic breast cancer, with a focus on controlling hematological toxicities. The scheduling regimen was first optimized offline for the first cycle, which led to a different scheduling than the standard of care. Then, the scheduling was adaptive for each patient and each cycle. It could be modified to avoid toxicities, based on data collected from monitoring neutrophil counts and individual predictions from the model. The study – called Model-I – was a success, with no grade ≥ 3 hematologic toxicity, and a doubling of the median overall survival compared to historical data with standard dosing (Figure 2).
Mechanistic learning for prediction of resistance to immune-checkpoint blockade
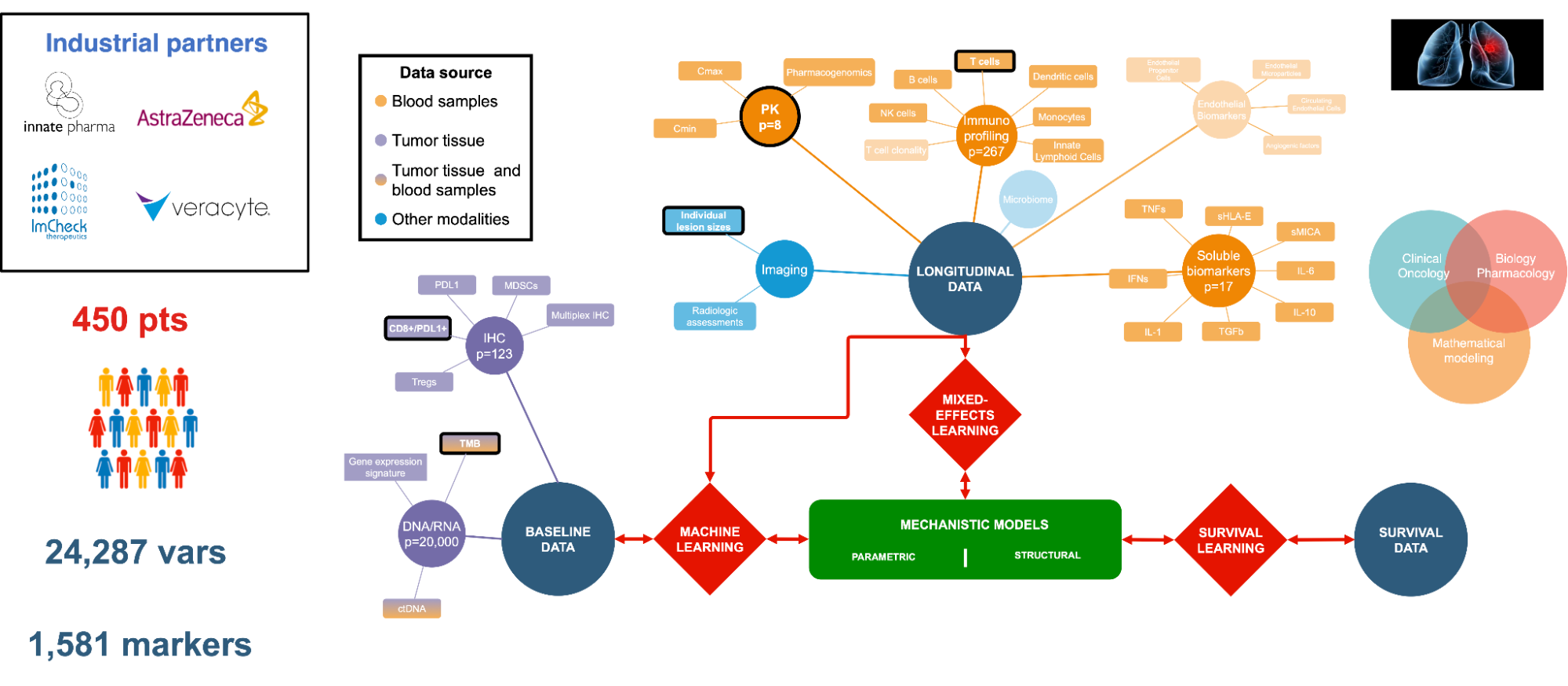
A major research project started in 2020 in COMPO and still ongoing consists of the statistical, machine and mechanistic learning analysis of data collected during the PIONeeR national RHU research project (Figure 3) [6,7]. The PIONeeR project is a large-scale national clinical study (hospital-university research project, funded with €10M) aimed at understanding and predicting resistance to immune checkpoint inhibitors (ICI) in advanced lung cancers. These treatments can lead to long-term remissions but only for 20-30% of patients. Extensive clinical and biological data were collected before and during treatment, making PIONeeR the largest dataset globally on this topic to date. The data is multi-scale, multi-modal, and longitudinal, covering tumor tissue and blood circulation. Significant efforts were made to automate the analysis of this vast dataset, including the development of open source R and python libraries for data preprocessing, automated biostatistics, machine learning and reporting, and continuous integration / continuous deployment pipelines. The project has led to the identification of a multivariate biomarker signature predicting ICI resistance, achieving an AUC of 0.78 and a balanced accuracy of 72%. The core packages developed during the project.
Mechanistic learning for prediction of survival and clinical trials outcome
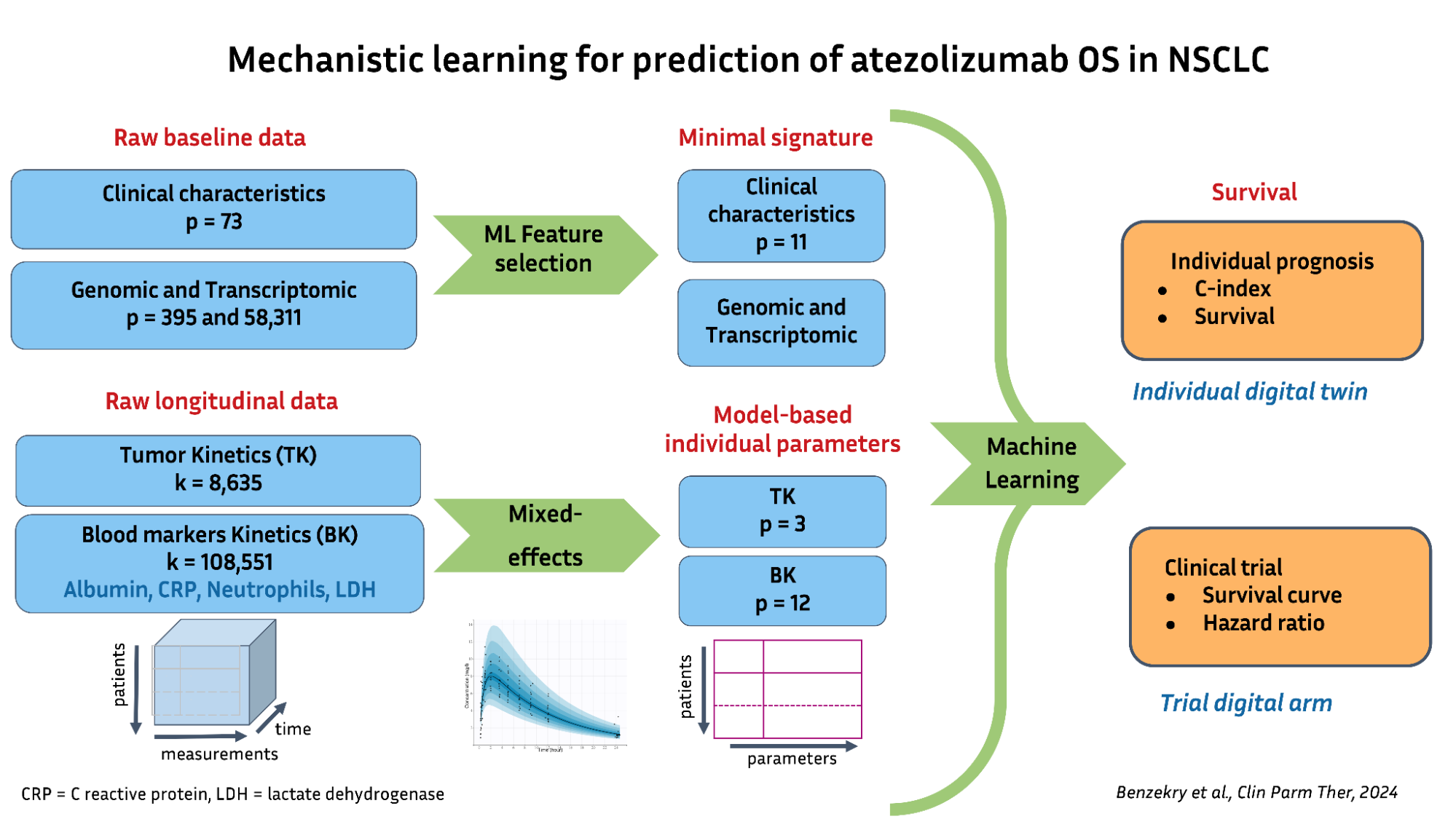
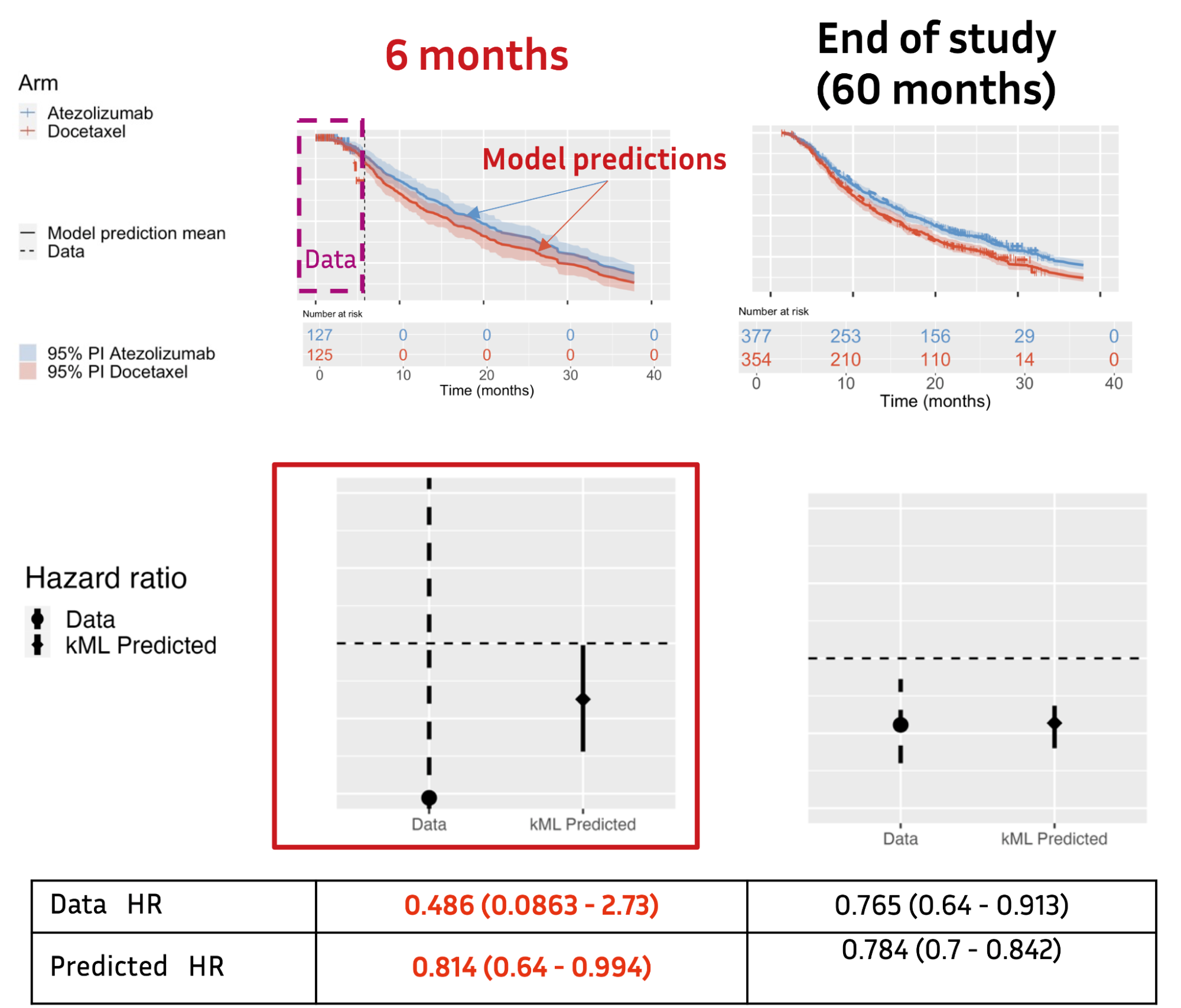
A recent project was performed in collaboration with Roche/Genentech. We developed models to predict the outcome of clinical trials in lung cancer immune-checkpoint blockade (ICB) treatments, using data from over 3,500 patients [8,9,10]. The main novelty was to go beyond classical modeling of only tumor kinetics (tumor growth inhibition models) and to integrate both tumor kinetics (TK) and routine blood markers’ kinetics (BKs) into a survival machine learning model (Figure 4). A first approach termed kinetics-Machine Learning (kML), based on empirical models for BKs for ICB monotherapy, was implemented within nlml_onco. The algorithm was trained on phase 2 trials (N=533 patients, ~ 130k BK time points) and tested on a phase 3 trial (N=377 and 354 in the two treatment arms). It outperformed the state-of-the-art, achieving a C-index of 0.8 and AUC of 0.9 for individual survival prediction.
More importantly, the model was able to accurately predict the outcome of the phase 3 trial using only early on-study data (Figure 5) [9]. We further moved to mechanistic modeling – and thus, mechanistic learning – for combination therapy, because the empirical models were found inappropriate. This gave not only a better understanding of the dynamics at stake but also predictions significantly improved compared to empirical modeling[10].
Mechanistic survival learning of metastatic relapse
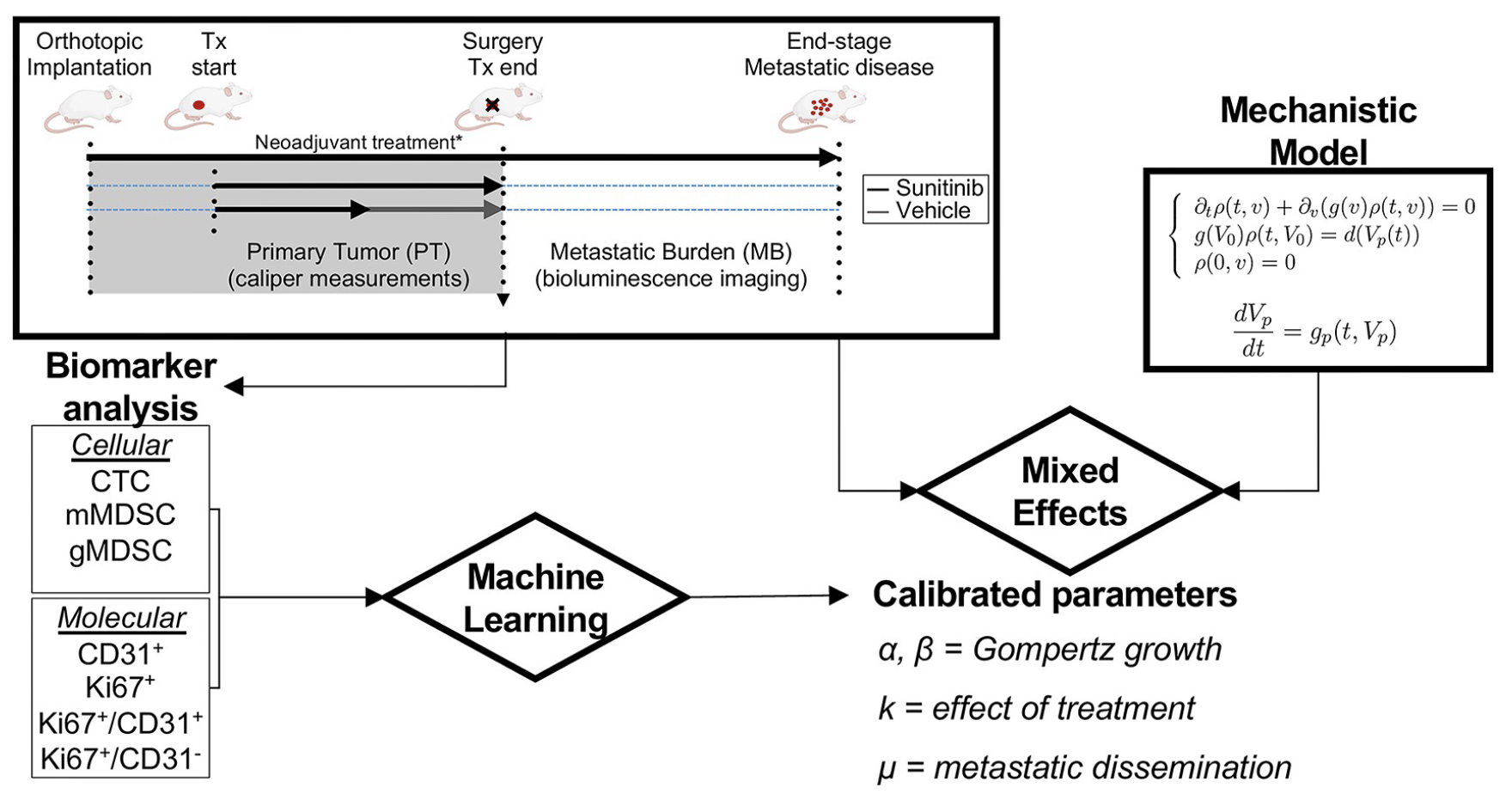
One key issue in treating patients with localized cancer, particularly breast cancer, is predicting potential metastatic relapse and estimating its timing. We developed mechanistic models of metastatic development using a size-structured partial differential equation. These models were carefully validated on multiple experimental datasets, including a recently released dataset from Dr. Ebos's lab (Figure 6) [11,12,13]. This dataset contains longitudinal data of primary and metastatic tumor growth in 251 mice subjected to different therapeutic regimens.
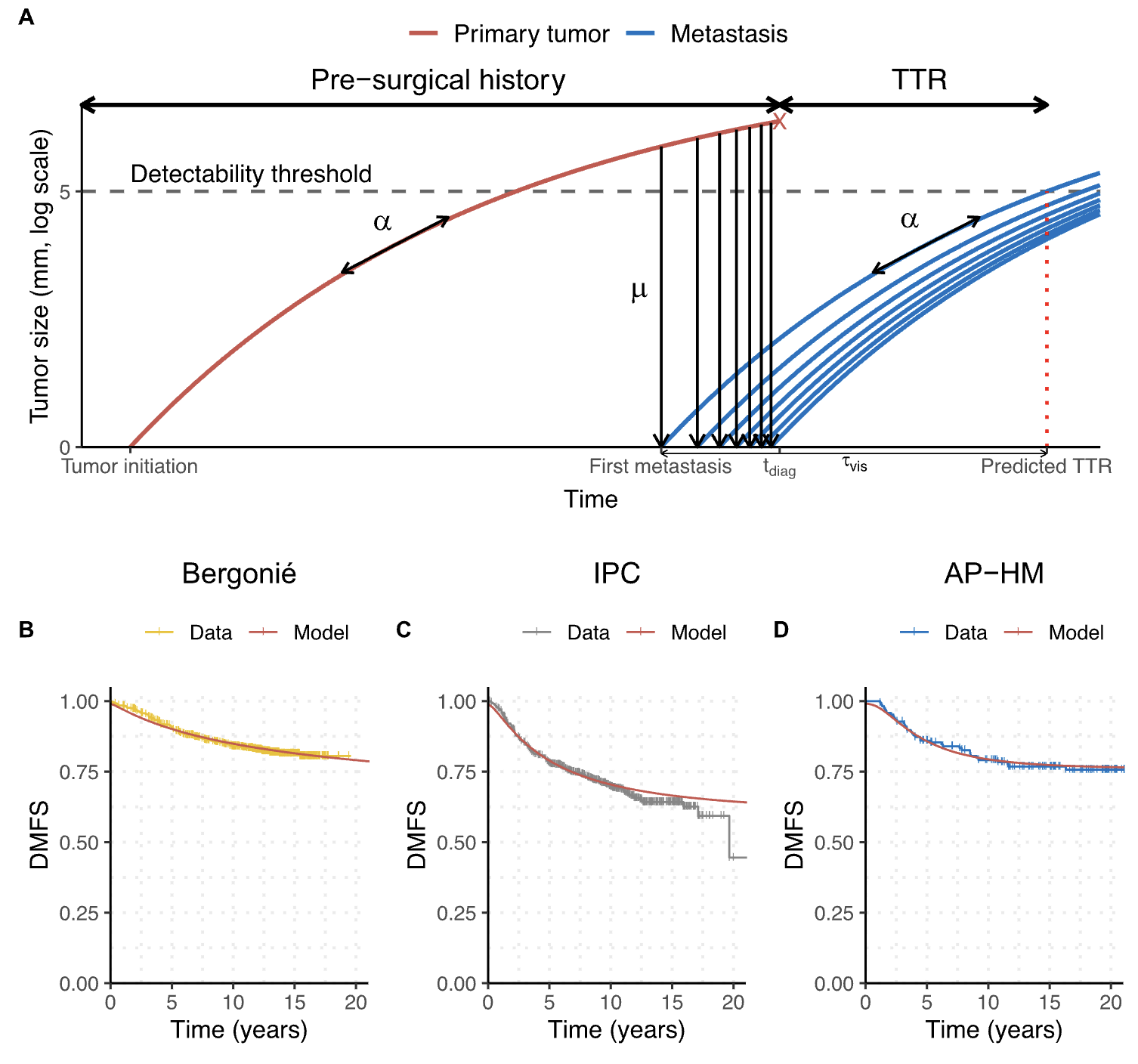
Then, using multiple clinical databases with over 1,000 patients, we proposed an original approach leveraging mixed-effects statistical models to exploit right-censored relapse data (Figure 7)[14,15]. This mechanistic learning approach for survival analysis allows to unravel the biological role of biomarkers, which cannot be achieved using statistical or purely ML approaches. Collaborating with oncologists and radiotherapists, we also applied the mathematical framework to brain metastases in non-small cell lung cancer [16,17].
We also are actively working on mechanistic learning for longitudinal fragmentome data from circulating free DNA during response to immunotherapy [18,19]; development and modeling of combined treatments with immunotherapy (either with nanoparticles or more classical systemic treatments); development of physiologically-based pharmacokinetic (PK) models and population PK and pharmacometrics for individualized dosing of chemotherapies, targeted therapies and immunotherapies.
Stay tuned for further news on exciting research projects!
For more info :References
- Benzekry, S. Artificial intelligence and mechanistic modeling for clinical decision making in oncology. Clin Pharmacol Ther 108 doi:10.1002/cpt.1951.
- Iliadis, A., Brown, A. C. & Huggins, M. L. APIS: a software for model identification, simulation and dosage regimen calculations in clinical and experimental pharmacokinetics. Computer Methods and Programs in Biomedicine 38 doi:10.1016/0169-2607(92)90103-e.
- Iliadis, A. & Barbolosi, D. Optimizing drug regimens in cancer chemotherapy by an efficacy-toxicity mathematical model. Comput. Biomed. Res. 33 , 211–226 (2000).
- Meille, C., Barbolosi, D., Ciccolini, J., Freyer, G. & Iliadis, A. Revisiting Dosing Regimen Using Pharmacokinetic/Pharmacodynamic Mathematical Modeling: Densification and Intensification of Combination Cancer Therapy. Clin Pharmacokinet 55 doi:10.1007/s40262-016-0374-7.
- Hénin, E., Meille, C., … Freyer, G. Revisiting dosing regimen using PK/PD modeling: the MODEL1 phase I/II trial of docetaxel plus epirubicin in metastatic breast cancer patients. Breast Cancer Res Treat 156 doi:10.1007/s10549-016-3760-9.
- Greillier, L., Monville, F., … Barlesi, F. Abstract LB120: Comprehensive biomarkers analysis to explain resistances to PD1-L1 ICIs: The precision immuno-oncology for advanced non-small cell lung cancer (PIONeeR) trial. Cancer Research 82 doi:10.1158/1538-7445.AM2022-LB120.
- Barlesi, F., Monville, F., … Benzekry, S. Comprehensive biomarkers (BMs) analysis to predict efficacy of PD1/L1 immune checkpoint inhibitors (ICIs) in combination with chemotherapy: a subgroup analysis of the Precision Immuno-Oncology for advanced Non-Small CEll Lung CancER (PIONeeR) trial. Ann Oncol 16 doi:10.1016/iotech/iotech100100.
- Benzekry, S., Karlsen, M., … Jamois, C. Supporting decision making and early prediction of survival for oncology drug development using a pharmacometrics-machine learning based model. in PAGE vol. 30 10276 (2022).
- Benzekry, S., Karlsen, M., … Jamois, C. Predicting Survival in Patients with Advanced NSCLC Treated with Atezolizumab Using Pre- and on-Treatment Prognostic Biomarkers. Clinical Pharmacology & Therapeutics 116 doi:10.1002/cpt.3371.
- Taieb, R., Bruno, R., Jin, J. & Benzekry, S. Mechanistic modelling of tumor kinetics coupled with biomarker dynamics for survival prediction in non-small cell lung cancer patients. in PAGE vol. 32 10812 (2024).
- Benzekry, S., Tracz, A., … Ebos, J. M. L. Modeling Spontaneous Metastasis following Surgery: An In Vivo-In Silico Approach. Cancer Res 76 , 535–547 (2016) doi:10.1158/0008-5472.CAN-15-1389.
- Benzekry, S., Mastri, M., Nicolò, C. & Ebos, J. M. L. Machine-learning and mechanistic modeling of metastatic breast cancer after neoadjuvant treatment. PLOS Computational Biology 20 , e1012088 (2024) doi:10.1371/journal.pcbi.1012088.
- Mastri, M., Benzekry, S. & Ebos, J. M. Pre- and post-surgical monitoring of experimental primary tumor growth and metastasis under neo-adjuvant treatment. (2024) doi:10.5281/zenodo.10607753.
- Nicolò, C., Périer, C., … Benzekry, S. Machine Learning and Mechanistic Modeling for Prediction of Metastatic Relapse in Early-Stage Breast Cancer. JCO Clin Cancer Inform 4 , 259–274 (2020) doi:10.1200/CCI.19.00133.
- Bigarré, C., Bertucci, F., … Benzekry, S. Mechanistic modeling of metastatic relapse in early breast cancer to investigate the biological impact of prognostic biomarkers. Computer Methods and Programs in Biomedicine 231 doi:10.1016/j.cmpb.2023.107401.
- Bilous, M., Serdjebi, C., … Benzekry, S. Quantitative mathematical modeling of clinical brain metastasis dynamics in non-small cell lung cancer. Sci Rep 9 doi:10.1038/s41598-019-49407-3.
- Benzekry, S., Schlicke, P., … Simon, E. Computational markers for personalized prediction of outcomes in non-small cell lung cancer patients with brain metastases. Clin Exp Metastasis 41 doi:10.1007/s10585-023-10245-3.
- Phuong, L. N., Salas, S. & Benzekry, S. Computational modeling for circulating cell-free DNA in clinical oncology. JCO Clinical Cancer Informatics (2025).
- Salas, S., Nguyen Phuong, L., … Benzekry, S. Long cell-free DNA fragments predict early-progression in patients with advanced or metastatic cancer treated with immune-checkpoint inhibition. JCO 42 , e14550–e14550 (2024) doi:10.1200/JCO.2024.42.16_suppl.e14550.
© 2026 - The Mathematical Oncology Blog