The biomarker conundrum for adaptive dosing/tumour control
…oh and that pesky cumulative risk!
Adaptive dosing is an approach which is designed to help control the tumour. It simply involves starting/stopping the treatment based on the level of tumour burden within a patient. You may be asking why would you want to control it, surely you want to just get rid of it especially if you are suffering from it, which most patients are. The reason is that you can’t truly get rid of the disease – all that happens eventually is that the disease is replaced by another one which cannot be treated. (Note, this doesn’t always happen.) Adaptive dosing involves using the disease you can kill to control the disease you can’t, since the disease you can kill is holding back the disease you can’t. Sounds like a sure-fire bet, I’m convinced here’s my house as a wager, but... Is there any empirical evidence that suggests this is worth pursuing? There are a couple of articles showing that in mice studies it may be beneficial. I will leave it you to decide how credible/believable these are. (Just take a note of the sample sizes in the earlier studies, lack of randomization, lack of blinding, lack of model identifiability, doses/concentrations not being clinically relevant.) What about clinical evidence? There is a single clinical trial involving a small number of patients published in quite a “prestigious” journal which can be found here. Again, I will let you decide how credible the comparisons the authors make are. (Just take note of the lack of details on known prognostic factors, lack of details on what they describe the contemporous cohort, defined as a matched cohort with no details, oh and the small issue of a selection bias when comparing to a clinical trial. We shouldn’t let poor trial reporting and bias get in the way of science though, see here for a letter that has been provisionally accepted.) So that’s the empirical evidence, are you still convinced? I’m still in, here’s my favourite pair of socks... What is the biomarker conundrum? Well it relates to the fact that there isn’t a biomarker that fully captures the treatment effect on the end-point of interest, see the diagram below:
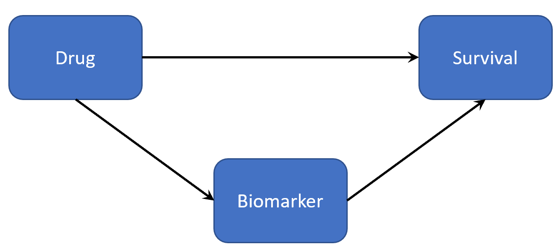 In the above diagram we have that drug effects biomarker, a measure of tumour burden, and biomarker effects patient survival. The biomarker here is a surrogate for the actual level of tumour burden, how much it truly captures is unknown it definitely won’t be all of it. There is another arrow which goes directly from drug to patient survival, why? The biomarker doesn’t always, in fact rarely, captures the entire treatment effect on the end-point. (If you are interested in the topic of surrogate biomarkers then a great starting point is the Prentice Criteria and numerous articles in the literature that cite the criteria.) That is most biomarkers are not drug independent surrogates.
A useful theoretical exercise for those advocating adaptive dosing would have been to explore how the strength of the relationships (correlations), in the above diagram, affect your adaptive dosing algorithm. In order to do that though you need to write down a model linking the biomarker to survival.
There is a huge array of empirical evidence which has shown that tumour burden measured in many ways is a time-dependent covariate in survival models. These survival models also account for the cumulative risk. What do those two statements mean? The probability of experiencing an event, death for example, in the next time interval is conditional on you surviving up to that current point in time but also on the current value of the tumour burden marker. (There is ~25 years of evidence on this in the statistical modelling literature, simply search for time-varying covariate or joint-longitudinal time-to-event models.) Once we consider this, see the article here, we cannot even begin to consider the above problem statement regarding surrogacy as we can’t even find an adaptive dosing algorithm which improves over continuous dosing. (Note, this does hold for all parameter value/initial conditions for the structural model chosen – just take a step back and think about the survival function in general and the empirical evidence from the statistical modelling community.) The theoretical models advocating adaptive dosing have failed to acknowledge cumulative risk and that tumour burden is a time-varying predictor of the end-point, probably because those advocating it are trying to become multi-disciplinary scientists – jack of all trades and masters of none! Would you get a plumber to re-wire your house?
In the above diagram we have that drug effects biomarker, a measure of tumour burden, and biomarker effects patient survival. The biomarker here is a surrogate for the actual level of tumour burden, how much it truly captures is unknown it definitely won’t be all of it. There is another arrow which goes directly from drug to patient survival, why? The biomarker doesn’t always, in fact rarely, captures the entire treatment effect on the end-point. (If you are interested in the topic of surrogate biomarkers then a great starting point is the Prentice Criteria and numerous articles in the literature that cite the criteria.) That is most biomarkers are not drug independent surrogates.
A useful theoretical exercise for those advocating adaptive dosing would have been to explore how the strength of the relationships (correlations), in the above diagram, affect your adaptive dosing algorithm. In order to do that though you need to write down a model linking the biomarker to survival.
There is a huge array of empirical evidence which has shown that tumour burden measured in many ways is a time-dependent covariate in survival models. These survival models also account for the cumulative risk. What do those two statements mean? The probability of experiencing an event, death for example, in the next time interval is conditional on you surviving up to that current point in time but also on the current value of the tumour burden marker. (There is ~25 years of evidence on this in the statistical modelling literature, simply search for time-varying covariate or joint-longitudinal time-to-event models.) Once we consider this, see the article here, we cannot even begin to consider the above problem statement regarding surrogacy as we can’t even find an adaptive dosing algorithm which improves over continuous dosing. (Note, this does hold for all parameter value/initial conditions for the structural model chosen – just take a step back and think about the survival function in general and the empirical evidence from the statistical modelling community.) The theoretical models advocating adaptive dosing have failed to acknowledge cumulative risk and that tumour burden is a time-varying predictor of the end-point, probably because those advocating it are trying to become multi-disciplinary scientists – jack of all trades and masters of none! Would you get a plumber to re-wire your house?
© 2026 - The Mathematical Oncology Blog