BIRS Recap: Biophysically-Constrained GBM Predictions via Deep-Learning Integrating Structural SINDY with Mechanistic Filters
Workshop Report (Mechanistic Learning as a combination of Machine Learning and Modeling in Mathematical Oncology. BIRS, Banff, CA, Jan 5-10, 2025)
This blog is one in a series resulting from the Winter 2025 BIRS workshop on Mechanistic Learning as a Combination of Machine Learning and Modeling in Mathematical Oncology.
Upon arriving to the snowy mountain landscape that is the Banff International Research Station (BIRS) in January 2025 for a workshop themed “Mechanistic Learning as a Combination of Machine Learning and Modeling”, 8 individuals who would go on to form Team DISS-MF (Deep- learning Integrating Structural Sindy with Mechanistic Filters) were assembled to find common interests and forge new frontiers in the wilderness of mathematics. This is our story.
After a stimulating and inspiring opening session to the workshop, our group gathered in the common area of the BIRS building and quickly realized that a majority of our team had active research in glioblastoma. With this starting point, we sought to integrate our expertise and computational tools into a unique framework that could advance our understanding and treatment of this devastating disease.
Glioblastoma multiforme (GBM) remains one of the most aggressive and challenging malignancies of the central nervous system, with a devastating prognosis despite advances in treatment protocols. The median overall survival for GBM patients is under 15 months following initial diagnosis, primarily due to tumor recurrence (Kwak et al., 2024; Stupp et al., 2005; Molinaro et al., 2020). Standard treatment approaches often fail to address the (radiologically invisible) infiltration of malignant cells into surrounding tissue (Akbari et al., 2016; Chang et al., 2007). Despite years of research, including from members in our team, the inherent variability exhibited by GBM means that no single imaging metric has proven adequate to accurately map tumor infiltration. We challenged ourselves to address this critical gap by integrating dynamic and structural brain imaging through a new concept in mechanistic learning that we refer to as “mechanistic filters”.
Mechanistic Filters as an effective means for multimodal data fusion
We began by identifying two essential elements of GBM treatment efficacy: tumor growth driven by tumor cell infiltration patterns, and drug distributions originating from intratumoral fluid flows. While each of these components had been previously modelled, we proposed to combine them with a new means of multimodal data fusion. We agreed to explore how to achieve this goal through mechanistic filtering within a neural network architecture. We aimed to ensure that the model predictions adhered to known biophysical constraints of GBM behavior, particularly regarding how fluid can flow through tissue, how tumor cells interact with different brain tissue types, and how they respond to the local microenvironment. This hybrid approach leverages both the pattern recognition capabilities of deep learning and biological mechanistic modeling. We hypothesized that this synergy results in more accurate and biologically plausible predictions of tumor recurrence locations.
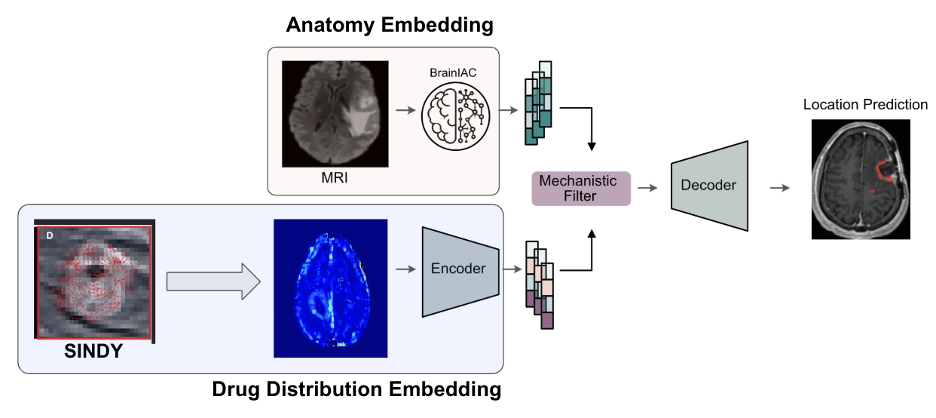
Our approach involved three key steps to integrate dynamic brain Magnetic Resonance Imaging (MRI, Figure 1): a neural network architecture to encode the brain anatomy aiming to describe GBM growth patterns, an approximation of the flow field to embed the expected drug distribution, and a mechanistic filter to combine data modalities prior to the reconstruction, i.e. prediction. In the following, we describe each of these steps.
1) Dynamic Brain Imaging and Flow Field Modeling
Interstitial fluid flow (IFF) field modeling represents a significant advancement in our understanding of brain tissue dynamics, particularly in the context of glioblastoma progression. Unlike static imaging techniques that capture only a snapshot of tumor morphology, flow field models characterize the dynamic nature of brain tissue, capturing both the spatial and temporal patterns of IFF and tumor cell migration. These models are particularly valuable for GBM, where understanding the complex movement of cancer cells through brain tissue is crucial for predicting recurrence patterns (Kwak et al., 2024).
Our idea has been to integrate the weak form of Sparse Identification of Nonlinear Dynamics (SINDY) (Brunton et al., 2016; Messenger & Bortz 2021) with multiparametric MRI data to construct detailed models of interstitial fluid flow fields. SINDY provides a mathematical framework for identifying the governing equations of complex dynamical systems from data (Alber et al., 2024; Cranmer et al., 2024), allowing us to characterize the spatiotemporal evolution of intratumoral IFF and GBM infiltration (Carmen et al. 2025). By applying polynomial basis functions to spatiotemporal brain imaging data, one can derive a measured state function that represents the underlying dynamics of fluid flow in the tissue (Woodall et al. 2024). This process transforms conventional MRI scans into dynamic models that capture where fluid is flowing in and around the tumor and provide information about where tumor cells may be located and how they are likely to move through surrounding brain tissue over time.
We studied the application of SINDY-based modeling to describe contrast agent dynamics in dynamic contrast-enhanced (DCE) MRI data of the brain, enabling us to estimate the spatiotemporal dynamics of drug concentration following its delivery to brain tissue. Our preliminary implementation employed a finite difference scheme in space and time. Using DCE data from a patient with glioblastoma, we extracted patient-specific flow parameters for contrast agent dynamics and applied these to estimate drug distribution patterns. The resulting simulations predicted drug distribution in the tissue, allowing us to calculate voxel-wise drug accumulation over time. These flow field and drug concentration maps serve as critical inputs to our future data analyses and predictive modeling using neural network architectures as a means of modelling the complex interplay of drug-induced cell death and tumor proliferation.
2) Brain anatomy embedding
We then explored the integration of the Brain Imaging Adaptive Core (BrainIAC), which is a foundation model of the brain trained on over 50,000 brain MRI scans that provides robust feature extraction capabilities for neuroimaging data. Of note, BrainIAC was developed and recently published by one of our team members, Divy Tak (Tak et al., 2024). We reasoned that the depth and scope of this foundation model would ensure that the network model approach could effectively and readily identify relevant imaging biomarkers/features within the complex and heterogeneous landscape of GBM presentations.
3) Mechanistic Filter Integration
In order to integrate the mechanistic model with the foundation model, we developed the concept of a “mechanistic filter.” The mechanistic filter is a critical innovation in our methodology, bridging data-driven neural network learning and biophysical understanding of glioblastoma behavior. Unlike traditional filtering operations that rely solely on pattern recognition, our mechanistic filter imposes physical constraints derived from known tumor biology, ensuring predictions remain biologically plausible even with limited training data. The filter implements the relationship
\[ f(v,c) = v(1-c^n)e^{-kc} \]
where tissue morphology (v) interacts with (local) drug distribution (c) according to established pharmacokinetic principles. This formulation enables the model to account for critical GBM- specific features, including the blood-brain barrier permeability variations around tumors, the differential infiltration rates through white versus gray matter, and the characteristic preference of GBM cells for migration along white matter tracts. By constraining the solution space of the neural network to physically realistic outcomes, we anticipate that mechanistic filters will improve prediction performance in a limited data setting, while simultaneously providing an interpretable fusion of the two input feature streams. This approach represents a novel combination of data science and mechanistic modeling, as it incorporates domain knowledge that would otherwise be difficult for a neural network to learn independently from limited clinical datasets.
Conclusion and Future Directions
Our pilot study at the BIRS workshop seeks to motivate translational potential of integrating neural networks with flow field modeling and mechanistic filters to predict GBM recurrence. By combining the pattern recognition capabilities of deep learning with the biophysical constraints of mechanistic modeling, we propose new means of mechanistic learning aiming to address typical limitations in the data science domain, such as limited data and model interpretability. The DISS-MF architecture may represent an advancement over previous approaches that relied solely on static imaging features, purely statistical models, fully mechanistic formulations that might oversimplify disease dynamics, or generalized, but non-mechanistic data interpretations.
Looking ahead, several promising directions arise from our perspectives. First, integrating additional data modalities, such as genomic and metabolomic profiles, could further enhance prediction accuracy by capturing the molecular drivers of tumor behavior. Second, longitudinal studies tracking patients through multiple treatment cycles could reveal how flow field patterns evolve in response to therapy, potentially enabling adaptive treatment planning. Longitudinal datasets would further enable estimation of other mechanistic fields of interest, such as proliferation, invasion, treatment efficacy maps (Wu et al.2022, Hormuth et al. 2021, Lorenzo et al. 2022). Finally, translating these predictions into actionable clinical interventions represents an ultimate goal—developing protocols for targeted radiation boost volumes, gross total surgical resection boundaries, or localized drug delivery based on recurrence predictions. As computational methods and imaging technologies continue to advance, we anticipate that the integration of dynamic mechanistic modeling with deep learning will become an increasingly powerful approach for addressing the persistent challenge of GBM recurrence.
References
- Akbari H, Macyszyn L, Da X, et al. (2016). Imaging surrogates of infiltration obtained via multiparametric imaging pattern analysis predict subsequent location of recurrence of glioblastoma. Neurosurgery, 78(4), 572-580. DOI: 10.1227/NEU.0000000000001202
- Alber M, Buganza Tepole A, Cannon WR, et al. (2019). Integrating machine learning and multiscale modeling—perspectives, challenges, and opportunities in the biological, biomedical, and behavioral sciences. npj Digital Medicine, 2(1), 1-11. DOI: 10.1038/s41746-019-0193-y
- Brunton SL, Proctor JL, Kutz JN. (2016). Discovering governing equations from data by sparse identification of nonlinear dynamical systems. Proceedings of the National Academy of Sciences, 113(15), 3932-3937. DOI: 10.1073/pnas.1517384113
- Chang EL, Akyurek S, Avalos T, et al. (2007). Evaluation of peritumoral edema in the delineation of radiotherapy clinical target volumes for glioblastoma. International Journal of Radiation Oncology, Biology, Physics, 68(1), 144-150. DOI: 10.1016/j.ijrobp.2006.12.009
- Hormuth, D. A., Al Feghali, K. A., Elliott, A. M., Yankeelov, T. E., & Chung, C. (2021). Image- based personalization of computational models for predicting response of high-grade glioma to chemoradiation. Scientific reports, 11(1), 8520. DOI: 10.1038/s41598-021-87887-4
- Tak D, Garomsa BA, Chaunzwa TL, et al. (2024). A foundation model for generalized brain MRI analysis, medRXiv, 2024.12.02.24317992. DOI: 10.1101/2024.12.02.24317992
- Kwak S, Akbari H, Garcia JA, et al. (2024). Predicting peritumoral glioblastoma infiltration and subsequent recurrence using deep-learning–based analysis of multi-parametric magnetic resonance imaging. Journal of Medical Imaging, 11(5), 054001. DOI: 10.1117/1.JMI.11.5.054001
- Lorenzo G, Jarrett AM, Meyer CT, et al. (2023). A global sensitivity analysis of a mechanistic model of neoadjuvant chemotherapy for triple negative breast cancer constrained by in vitro and in vivo imaging data. Engineering with Computers, 40(3), 1469-1499. DOI: 10.1007/s00366-023-01873-0
- Messenger DA & Bortz DM (2021). Weak SINDY: Galerkin-Based Data-Driven Model Selection. Multiscale Modeling and Simulation, 19(3):1474–1497. DOI: 10.1137/20M1343166
- Molinaro AM, Hervey-Jumper S, Morshed RA, et al. (2020). Association of maximal extent of resection of contrast-enhanced and non-contrast-enhanced tumor with survival within molecular subgroups of patients with newly diagnosed glioblastoma. JAMA Oncology, 6(4), 495-503. DOI: 10.1001/jamaoncol.2019.6143
- Stupp R, Mason WP, van den Bent MJ, et al. (2005). Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. New England Journal of Medicine, 352(10), 987-996. DOI: 10.1056/NEJMoa043330
- Woodall RT, Esparza CC, Gutova M, et al. (2024). Model discovery approach enables noninvasive measurement of intra-tumoral fluid transport in dynamic MRI. APL Bioeng. AIP Publishing, 8(2), 026106. DOI: 10.1063/5.0190561
- Wu C, Jarrett AM, Zhou Z, et al. (2022). MRI-based digital models forecast patient-specific treatment responses to neoadjuvant chemotherapy in triple-negative breast cancer. Cancer Research, 82(18), 3394-3404. DOI: 10.1158/0008-5472.CAN-22-1329
© 2026 - The Mathematical Oncology Blog